Posted by Padmaja Pati and Sanjina Gupta
As we usher in the International Day for Sexual and Reproductive Health Awareness, we, two individuals identifying as women and possessing uteri, wanted to delve a little deeper into how our bodies have been the battle ground of control in this patriarchal society and state at large for centuries on end.
Bodies with uteri have always been a site of asserting control, policing, imposing limitations in the name of ‘population control’, ‘family planning’ or ‘women empowerment’, and it is baffling to witness normalisation, acceptance or hushing up of such violations of autonomy and agency of these individuals. In the realm of this discourse, it is critical to understand how these violations take place towards bodies that are marginalised and vulnerable, and try to reflect on what sort of consequences such violations will have if the bodies affected were to belong to those of an upper caste, class or a cis-male gender.
While talking about how State and society have been imposing decisions on our bodies in the name of development, we wanted to take a look at how family planning as a government endorsed programme has been at the centre of many laws, policies and schemes in India since independence and how different approaches have been used to arrest the growing population or as we commonly know it as population ‘control’.
Moreover, it will be interesting to see how the population is being ‘controlled’ by controlling marginalised bodies, who are often looked at as insignificant, dispensable and voiceless in our socio-economic context. The common notion that marginalised communities hailing from a certain class, caste and religion make ‘more’ children than the upper class, upper caste people from the majority religion has been one of the few reasons where government’s family planning schemes have repeatedly targeted such communities.
Here two things are important to note in this conversation:
- How sexual rights of a certain community are under scrutiny, and
- How sexuality and sexual rights of a certain gender in that community are under scrutiny
Despite working in the SRHR space, we were unaware of the gross degree of certain violations. In our conversations with women from marginalised communities in West Bengal, we kept hearing stories where long term contraceptive methods like IUCDs have been installed in their bodies without seeking their consent. Digging up more articles and reportage available on this unethical practice revealed that it has been going on since a long time. The narrative that a poor, lower caste community has no other recreation other than procreation has driven our country’s family planning programs for ages.
Moreover, this biased outlook has led not just to violations and misconducts from the service providers’ part but also destroyed the entire essence of family planning, which at its core wants to promote a healthy sexual and reproductive life for all individuals. India is also signatory to the ICPD PoA of 1994 which was a watershed moment in development work and stated that we need to move away from demographic targets and respect, protect and fulfill individual sexual and reproductive lives.
Bodies with uteri have always been a site of asserting control, policing, imposing limitations in the name of ‘population control’, ‘family planning’ or ‘women empowerment’, and it is baffling to witness normalisation, acceptance or hushing up of such violations of autonomy and agency of these individuals.
Radha (name changed), based in West Bengal is a married 23-year-old who underwent a c-section two years ago at a government facility. When she was discharged, she found that an IUCD had been inserted into her uterus without any prior consent either from her or her family. On protesting, she was told by the nurse that it was done for her ‘benefit’ and then the nurse humiliated her further by saying that the IUCD would save her from visiting the hospital next month with another pregnancy, taking a dig at her by assuming that she or her husband were not responsible enough to use any contraception.
For more than a year, Radha endured excruciatingly painful menstrual cycles where she would bleed twice a month, and would not be able to leave her bed while also nursing an infant alongside. After 13 months of suffering, she got the IUCD removed by a registered practitioner with the help of a local social welfare organisation. In addition, she willingly opted for one of the alternative contraceptive methods that were offered to her.
Radha’s story is one among many others who faced similar predicaments. The official reference manual of IUCD services clearly states that verbal consent is needed from the patients before the childbirth. And they are to be counselled about the advantages, limitations, effectiveness and possible side effects or complications of the IUCD prior to delivery. However, the reality is that in many instances neither proper consent is taken nor is after-care provided to these women, who are left to deal with the repercussions of such violations on their own.
Also read: 5 Myths About Population Control In India That Need To Be…
Since its inception in 1952, family planning has been about controlling the bodies of people with uteri. Starting with the first ever initiative when women were asked to follow a “rhythm method” where they were given beaded necklaces to determine their safe days to the present situation of imposing long term contraceptives and sterilisations over bodies with uteri it has been a long and rocky road. A close look at the National Family Health Survey-4 data corroborates the above discussed observation. It reveals that out of 47.8 percent of the total modern contraception methods that are in current use in our country, 41.6 percent are subjected to the bodies of a certain gender—women or bodies with uteri.
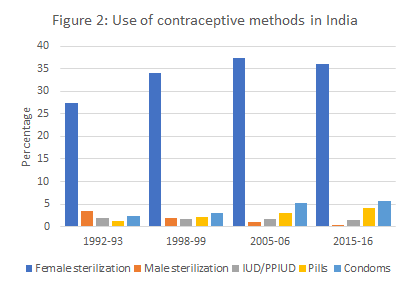
While usage of condoms and vasectomy or male sterilisation does occupy a seat among these modes of contraception (condom use = 5.6 percent and male sterilisation = 03 percent), the numbers are a witness of who is the one having to bear the burden of contraception.
According to sexual and reproductive health service providers and policy designers, the myths and biases surrounding use of condoms and vasectomy are one of the major deterrents.
So, why this glaring disparity?
According to sexual and reproductive health service providers and policy designers, the myths and biases surrounding use of condoms and vasectomy are one of the major deterrents. Although the non-scalpel vasectomy used nowadays is no more painful than an injection and although it is meant to be permanent it can be reversed surgically, the patriarchal notions of masculinity and the myth that the procedure will somehow affect erection and sexual pleasure, as well as the continued impact of the forced vasectomy programme imposed during the Emergency period in the 1970s, means that men are extremely reluctant to adopt this very effective and minimally invasive method while women continue to throng sterilization camps which can often be dangerous and have repeatedly resulted in deaths.
Also read: Why Endogamous Marriages Could Make Us An Unhealthy Population
All these discussions leave us with a set of burning questions to ponder upon: what makes women or bodies with uteri so easy to regulate and control? Why do they carry this burden? Is it because of their ability to give birth or is it about the social standing they have in this patriarchal society or both? Does the burden of saving the family from unwanted expenses (more mouths to feed) increase exponentially as one gets pushed to the margins of the society?
Access to effective family planning and contraception can contribute greatly to gender equality and women’s empowerment by allowing them to have control over their bodies and fertility. However, in many parts of our country forced sterilisations, hysterectomies, forced insertion of IUCD have been taking place right under the surveillance of service providers and State, whether it is forced hysterectomies in Maharashtra’s Beed district or 14 women dying at sterilisation camps in Chhattisgarh or the recently out cases of non-consensual insertion of IUDs after childbirth in Kolkata, West Bengal.
Moreover, concerned authorities try to justify their coercive actions with various reasons such as undisrupted labour supply, population control, family planning, lessened economic burden so on and so forth. However, these violations do have consequences. They negatively impact the physical, mental, and socio-cultural well-being of the people whose rights to bodily autonomy, privacy and information were or are being breached. Implementation of family planning methods in such a forced way widens the existing gender disparity, and pushes individuals already at the margins further into conformity towards subservient gender roles. So, does the State really care for us or are we just a number to be managed?
Note: There are also a range of similar violations for individuals identifying as non/binary or trans men in across states, however, not many of these go reported or been undocumented so far. Hence we have tried to use inclusive terms.
We would like to extend our gratitude to FII and ASAP for their support.
Sanjina is the founder and executive director of Rangeen Khidki Foundation. Sanjina holds a Masters degree in sociology and has a collective experience of 7 years in the social development sector.
Padmaja Pati is Research Manager with Rangeen Khidki Foundation. Padmaja is a mixed-method researcher in the field of education, gender, and food security with a master’s degree in Financial Economics.
Rangeen Khidki Foundation is a feminist youth led organisation based in Kolkata working in the space of sexual and reproductive health and rights. You can find them on their Website, Instagram, Facebook and LinkedIn.
Featured Image Source: Scroll